| Treatment of Refractory Status Epilepticus in Children |
|
| 부산대학교 어린이병원 소아청소년과 이윤진 |
|
 |
I. 서론
뇌전증지속상태(status epilepticus, SE)는 단순하게는 ‘뇌전증발작이 지속하는 상태’로 정의할 수 있다. SE가 다른 발작(seizure)과 다른 이유는, 일반적인 발작이 자기한정 에피소드(self-limiting episode)로 대부분 수 분 이내에 저절로 멈추고 발작 후 일정기간 불응기를 보이며 회복하는 반면에 SE는 발작이 지속하거나 의식 회복이 없이 발작이 반복하는 상태이기 때문이다. 따라서 SE의 병태생리는 자기한정 기능이 소실된 상태로 보아야 하며, 뇌의 신경학적인 결손 또는 생리적 변화를 가져오고 그 결과로 뇌손상이나 사망에 이를 수도 있어 신경계 |
응급질환으로, 빠른 진단과 치료의 시작이 필요하다. SE는 소아의 가장 흔한 신경학적 응급상황으로 연간 십만명 소아당 18-23례의 발병률을 보인다. SE의 발생빈도는 특징적인 두봉우리형(bimodal pattern)을 보여 1세 이하나 60세 이상에서 흔하다. 소아에서는 감염과 고열이 흔하며 부적절한 항뇌전증약의 복용이나 선천기형도 흔한 원인이다. 소아 SE의 20-28%는 열성경련에 의하며 이때는 전신강직간대발작의 빈도가 높다.
1997년 국제뇌전증퇴치기구(International League Against Epilepsy)에서는 SE를 ‘30분 이상 지속적인 발작 또는 30분 이상 의식 회복이 없이 반복하는 발작의 연속’이라고 정의하였다. 그러나 전신발작이 3분 이상 지속하는 경우가 극히 드물고, SE기간이 길수록 결과가 나쁘다는 등의 이유로 최근에는 5분 이상 지속하는 발작이나 의식 회복 없이 반복하는 2회 이상의 발작을 SE 정의로 제안하고 있다. 지속적인 SE 상태를, 초기 SE (early SE, 5-30분), 확립된 SE (established SE, >30분), 혹은 난치 SE (refractory SE, RSE, 2-3개 항경련제의 적정량 사용에도 SE 지속상태)로 구분하고 있다. SE의 단계적인 치료과정을 지칭하는 용어로써, 기존에 사용하던 1차, 2차, 3차 단계 약물에서, 응급(emergent), 긴급(urgent), 및 난치(refractory)라는 용어를 최근에 제시하고 있다.
SE로 인한 사망률은 5~50%로 다양하게 보고된다. 특히 강직 혹은 근간대 SE는 저산소증과 관계되는 경우가 많아 예후가 불량하다. SE의 예후는 발작의 적절한 치료 뿐만 아니라 빠른 원인 질환의 진단과 치료, 더불어 SE로 인한 뇌손상의 예방 등 여러 요인에 의하여 좌우되므로 SE의 기간을 최소화하고 원인 질환에 대한 정확히 파악 및 신속한 처치가 예후를 향상시키는데 열쇠이다.
II. 뇌전증지속상태에 대한 응급 대처 및 원인에 대한 평가
SE의 치료는 다른 중환자와 같이 기도 및 혈압유지가 중요하다. 경한 저산소증으로도 뇌가 쉽게 손상을 받을 수 있는 상태이고, 정맥주사하는 항경련제가 호흡부전을 초래할 수 있기 때문에 호흡관리가 특히 중요하다. 첫 2분 이내 비침습적인 기도유지, 호흡상태 및 활력징후를 평가한다. 첫 5분이내에 신경학적 진찰 및 말초정맥 확보 후, 응급단계 항경련제 주입을 시행한다. 환자 상태에 따라 필요하다면 기도삽관을 10분 이내 시행한다. SE 초기에는 혈압이 오르다가 15~30분이 경과하면서 혈압이 감소하는데, 이때 뇌혈류 유지를 위해 혈압을 적절하게 유지하는 것이 매우 중요하다.
상기의 응급 대처와 함께 가역적인 원인을 파악하여 원인질환의 치료까지 같이 진행하게 된다. 여러가지 혈액검사, 대사질환 검사, 뇌파 검사 및 신경영상검사(뇌 CT, MRI)를 시행하게 된다 (표 1~2). 의식이 혼미한 모든 환자에게서 SE를 의심하고 뇌파를 시행하여 적절한 진단을 내리는 것이 SE 치료의 시작이다. 뇌파는 초기 진단 뿐 아니라, 환자의 예후판정에 도움을 준다. 임상적으로 발작이 조절된 이후에도 뇌파에서 발작파가 지속되는 경우가 약 20% 있으므로, 임상적으로 발작이 멈추었더라도 SE 종료된 후 30분 이상의 지속적인 뇌파기록을 권유하고 있다.
III. 뇌전증지속상태(SE)의 치료
SE에서 항경련제는 정맥투여가 원칙이다 (표 1). Benzodiazepine 은 강력하고 효과적인 항경련제로 lorazepam 이 대표적이다. Lorazepam은 2~3회까지 반복토여가 가능한데, lorazepam을 투여한 후에도 SE가 지속되면 phenytoin (혹은 fosphenytoin) 을 20 mg/kg 정맥부하하고, 그래도 SE 상태가 지속되면 phenytoin 5~10 mg/kg 을 추가로 투여한다. 또는 barbiturate 가 주로 사용된다. 기존 심장질환이 있는 환자에서는 phenytoin을 투여하지 않는 것이 좋은데, 혈압이 90/60 이하로 떨어지거나, QT 간격이 증가하거나, 부정맥이 나타나면 주입 속도를 줄인다. SE 치료를 위해 약을 선택하는데 있어서, 알려진 부작용(표 3) 및 주의 사항에 따라 조절하도록 한다. 최근에는 심혈관계 부작용이 적고 효과는 유사한 valproate를 정맥 요법을 선택하기도 하며, levetiracetam 이나 topiramate 등을 고용량으로 정맥주사 혹은 경구투여하기도 한다.
IV. 난치 뇌전증지속상태(Refractory SE, RSE)의 치료(그림 1)
Benzodiazepine과 phenytoin과 같이 2가지 이상의 항경련제를 적정용량 투여 후에도 발작이 계속되면 난치 SE (RSE)로 판단한다. RSE에는 과거 phenobarbital을 흔히 사용하였으나, 최근에는 midazolam이나 propofol 등 정맥마취제 또한 사용하고 있다. Midazolam 이나 propofol 등은 부하용량 후에 지속적인 정맥주사를 하는데, RSE의 조절된 상태 및 뇌파를 고나찰하면서 용량을 조절한다. 이 단계에서도 발작이 조절되지 않으면, pentobarbital (thiopental) 정맥주사나 흡입마취제를 이용한 전신마취 등이 사용된다 (그림 1).
RSE 상태에서 최근에 시도하는 다른 약물들로 lidocaine, verapamil, ketamine, 및 magnesium가 알려져 있다. 비약물적 치료방법으로, 케톤생성식이요법, immunomodulation, 저체온요법, 뇌전증수술, 미주신경자극술, 반복경두개자기자극술, 및 전기경련요법 또한 시도 가능한 치료 방법들로, 각각의 장단점을 고려하여 치료계획을 결정하게 된다(표 4, 그림 1).
V. 참고문헌
1) Smith DM, McGinnis EL, Walleigh DJ, Abend NS. Management of Status Epilepticus in Children. J Clin Med. 2016 Apr 13;5(4).
2) Trinka E, Cock H, Hesdorffer D, Rossetti AO, Scheffer IE, Shinnar S, et al. A definition and classification of status epilepticusReport of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia. 2015 Oct;56(10):1515-23.
3) Abend NS, Loddenkemper T. Pediatric status epilepticus management. Curr Opin Pediatr. 2014 Dec;26(6):668-74. 4) Abend NS, Bearden D, Helbig I, McGuire J, Narula S, Panzer JA, et al. Status epilepticus and refractory status e
pilepticus management. Semin Pediatr Neurol. 2014 Dec;21(4):263-74.
5) Abend NS, Loddenkemper T. Management of pediatric status epilepticus. Curr Treat Options Neurol. 2014 Jul;16(7):301.
6) Venkatesan A, Tunkel AR, Bloch KC, Lauring AS, Sejvar J, Bitnun A, et al. International Encephalitis Consortium. Case definitions, diagnostic algorithms, and priorities in encephalitis: consensus statement of the international encephalitis consortium. Clin Infect Dis. 2013 Oct;57(8):1114-28.
7) Brophy GM, Bell R, Claassen J, Alldredge B, Bleck TP, Glauser T, et al. Neurocritical Care Society Status Epilepticus Guideline Writing Committee. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012 Aug;17(1):3-23.
8) Rossetti AO, Lowenstein DH. Management of refractory status epilepticus in adults: still more questions than answers. Lancet Neurol. 2011 Oct;10(10):922-30.
9) Abend NS, Gutierrez-Colina AM, Dlugos DJ. Medical treatment of pediatric status epilepticus. Semin Pediatr Neurol. 2010 Sep;17(3):169-75.
10) 대한뇌전증학회. 임상뇌전증학. 범문에듀케이션. 2013.
Table 1. Status epilepticus (SE) evaluation and management pathway. (Adapted from Abend and Loddenkemper and Abend et al.)
Immediate Management
Non-invasive airway protection and gas exchange with head positioning if needed.
Monitor oxygen saturation, blood pressure, heart rate, temperature.
Finger stick blood glucose.
Peripheral IV access.
Medical and neurologic examination.
Labs including basic metabolic panel, calcium, magnesium, CBC, LFT, coagulation tests, arterial blood gas, and anticonvulsant levels.
Evaluation for specific immediate reversible causes of seizures: hyponatremia, hypoglycemia, hypocalcemia, hypomagnesemia, and malignant hypertension.
Emergent Initial Therapy
IV Access:
Lorazepam 0.1 mg/kg (max 4 mg) may repeat in 5-10 min if seizures persist.
Diazepam 0.15-0.2 mg/kg IV (max 10 mg) may repeat in 5 min
No IV Access:
Diazepam, Rectal 2-5 yrs 0.5 mg/kg, 6-11 yrs 0.3 mg/kg, >12 yrs 0.2/kg (max 20 mg)
Midazolam, IM (13-40 kg=5 mg; >40kg=10mg), intranasal (0.2 mg/kg), Buccal (0.5 mg/kg)
Consider whether out-of-hospital benzodiazepines have been administered when considering how many doses to administer.
Urgent Management
Additional diagnostic testing as indicated:
Lumbar puncture (opening pressure, cell count with diff, protein, glucose, gram stain and culture)
Consider: oligoclonal band profile, IgG index, IgG synthesis rate, fungal culture,
herpes simplex virus PCR, enterovirus PCR, parechovirus PCR
Imaging: CT, MRI
Consider: toxicology lab, inborn error of metabolism, anti-thyroid peroxidase Ab,
anti-thyroglobulin Ab, bacterial cultures
Consider EEG monitoring to evaluate for psychogenic SE or persisting EEG-only seizures after convulsive SE terminates.
Neurology Consultation
Urgent Control Therapy
Phenytoin 20 mg/kg/ IV (may give another 5-10 mg/kg/ if needed)
OR Fosphenytoin 20 PE/kg IV (may give another 5-10 PE/kg if needed) (PE=phenytoin equivalents)
OR consider phenobarbital, valproate sodium, or levetiracetam
If <2 years, consider pyridoxine (100 mg IV)
|
Refractory Status Epilepticus (RSE) Management
If seizure continue after benzodiazepines and a second anti-seizure medication, the patient is in RSE regardless of elapsed time.
Continue management as plan for ICU admission/transfer and likely continuous EEG monitoring
Administer another Urgent Control anticonvulsant or proceed to pharmacologic coma.
Levetiracetam 20-60 mg/kg IV
Valproate sodium 20-40 mg/kg IV
Phenobarbital 20-40 mg/kg IV (may give another 5-10 mg/kg)
Pharmacologic Coma Medications
Midazolam 0.2 mg/kg bolus (max 10 mg) and then initiate infusion at 0.1 mg/kg/hr.
Pentobarbital 5 mg/kg bolus and then initiate infusion at 0.5 mg/kg/hr.
For both drugs, if dose escalation is needed, then re-bolus and do not increase infusion rate.
Propofol 2 mg/kg bolus and then infusion at 2-5 mg/kg/hr (up to 10 mg/lg/hr)
Pharmacologic Coma Management
Titrate to either seizure suppression or burst suppression based on continuous EEG monitoring.
Continue pharmacologic coma for 24-48 hrs.
Modify anti-seizure medications so additional coverage is in place for infusion wean.
Continue diagnostic testing and implementation of etiology directed therapy.
Add-on Options
Medications: phenytoin, phenobarbital, levetiracetam, valproate sodium, topiramate, lacosamide,
ketamine, pyridoxine, pyridoxal-5-phosphate, folinic acid, biotin
Other: epilepsy surgery, ketogenic diet, vagus nerve stimulator, immunomodulatory therapy
(methylprednisolone, IVIG, plasma exchange), hypothermia, electroconvulsive therapy.
|
Table 1. Status epilepticus (SE) evaluation and management pathway. (Adapted from Abend and Loddenkemper and Abend et al.)
Immediate Management
Non-invasive airway protection and gas exchange with head positioning if needed.
Monitor oxygen saturation, blood pressure, heart rate, temperature.
Finger stick blood glucose.
Peripheral IV access.
Medical and neurologic examination.
Labs including basic metabolic panel, calcium, magnesium, CBC, LFT, coagulation tests, arterial blood gas, and anticonvulsant levels.
Evaluation for specific immediate reversible causes of seizures: hyponatremia, hypoglycemia, hypocalcemia, hypomagnesemia, and malignant hypertension.
Emergent Initial Therapy
IV Access:
Lorazepam 0.1 mg/kg (max 4 mg) may repeat in 5-10 min if seizures persist.
Diazepam 0.15-0.2 mg/kg IV (max 10 mg) may repeat in 5 min
No IV Access:
Diazepam, Rectal 2-5 yrs 0.5 mg/kg, 6-11 yrs 0.3 mg/kg, >12 yrs 0.2/kg (max 20 mg)
Midazolam, IM (13-40 kg=5 mg; >40kg=10mg), intranasal (0.2 mg/kg), Buccal (0.5 mg/kg)
Consider whether out-of-hospital benzodiazepines have been administered when considering how many doses to administer.
Urgent Management
Additional diagnostic testing as indicated:
Lumbar puncture (opening pressure, cell count with diff, protein, glucose, gram stain and culture)
Consider: oligoclonal band profile, IgG index, IgG synthesis rate, fungal culture,
herpes simplex virus PCR, enterovirus PCR, parechovirus PCR
Imaging: CT, MRI
Consider: toxicology lab, inborn error of metabolism, anti-thyroid peroxidase Ab,
anti-thyroglobulin Ab, bacterial cultures
Consider EEG monitoring to evaluate for psychogenic SE or persisting EEG-only seizures after convulsive SE terminates.
Neurology Consultation
Urgent Control Therapy
Phenytoin 20 mg/kg/ IV (may give another 5-10 mg/kg/ if needed)
OR Fosphenytoin 20 PE/kg IV (may give another 5-10 PE/kg if needed) (PE=phenytoin equivalents)
OR consider phenobarbital, valproate sodium, or levetiracetam
If <2 years, consider pyridoxine (100 mg IV)
|
Refractory Status Epilepticus (RSE) Management
If seizure continue after benzodiazepines and a second anti-seizure medication, the patient is in RSE regardless of elapsed time.
Continue management as plan for ICU admission/transfer and likely continuous EEG monitoring
Administer another Urgent Control anticonvulsant or proceed to pharmacologic coma.
Levetiracetam 20-60 mg/kg IV
Valproate sodium 20-40 mg/kg IV
Phenobarbital 20-40 mg/kg IV (may give another 5-10 mg/kg)
Pharmacologic Coma Medications
Midazolam 0.2 mg/kg bolus (max 10 mg) and then initiate infusion at 0.1 mg/kg/hr.
Pentobarbital 5 mg/kg bolus and then initiate infusion at 0.5 mg/kg/hr.
For both drugs, if dose escalation is needed, then re-bolus and do not increase infusion rate.
Propofol 2 mg/kg bolus and then infusion at 2-5 mg/kg/hr (up to 10 mg/lg/hr)
Pharmacologic Coma Management
Titrate to either seizure suppression or burst suppression based on continuous EEG monitoring.
Continue pharmacologic coma for 24-48 hrs.
Modify anti-seizure medications so additional coverage is in place for infusion wean.
Continue diagnostic testing and implementation of etiology directed therapy.
Add-on Options
Medications: phenytoin, phenobarbital, levetiracetam, valproate sodium, topiramate, lacosamide,
ketamine, pyridoxine, pyridoxal-5-phosphate, folinic acid, biotin
Other: epilepsy surgery, ketogenic diet, vagus nerve stimulator, immunomodulatory therapy
(methylprednisolone, IVIG, plasma exchange), hypothermia, electroconvulsive therapy.
|
Table2. Suggested Infectious Disease Evaluation for Children with Refractory Status Epilepticus (RSE) (Adapted from Venkatesan et al. and McGuire and Greene)
Urgent Evaluation
1) Cerebrospinal fluid
Collect up to 10-20-mL CSF for immediate analysis and freeze remainder for later testing
Opening pressure on lumbar puncture
White blood cell count with differential, red blood cell count, and protein and glucose levels
Gram stain, bacterial culture, and fungal cultures (if immunocompromised)
PCR: herpes simplex virus (HSV) 1/2, enterovirus, and parechovirus (if age < 3 years)
2) Serum
Basic studies: CBC with differential, electrolytes and liver function, coagulation studies
Bacterial cultures
Serologies: Epstein-Barr virus (VCA IgG and IgM and EBNA IgG), Mycoplasma pneumoniae
Hold acute serum and collect convalescent serum 10-14 d later for paired antibody testing
3) Other samples
Mycoplasma pneumoniae PCR from throat swab
Enterovirus PCR and culture of throat and stool
4) Radiology
MRI of the brain with and without gadolinium
Chest imaging (chest x ray or CT or both)
If RSE persists without clear etiology for ≥ 24 hr, consider adding,
1) Cerebrospinal fluid
CSF serologies (IgM/IgG): HSV, human immunodeficiency virus, arboviruses (including St. Louis encephalitisvirus, California encephalitis group, eastern equine encephalitis virus, western equine encephalitis virus, and West Nile virus), and lymphocytic choric meningitis.
Acid fast bacilli (AFB) smear and Mycobacterium tuberculosis culture
PCR: Epstein-Barr virus, cytomegalovirus, human herpes virus (HHV) 6, and rotavirus
Oligoclonal bands and IgG index
Consider repeat HSV 1/2 testing 3-7 d after initial test if clinical suspicion remains
2) Serum
Serologies: adenovirus, arbovirus panel (including St. Louis encephalitisvirus, California encephalitis group, eastern equine encephalitis virus, western equine encephalitis virus, and West Nile virus), lymphocytic choric meningitis, HHV6, Borrelia sp., Toxoplasma gondii, and influenza.
Human immunodeficiency virus serology (consider RNA)
PCR: HSV 1/2 and varicella zoster virus
3) Other samples
Consider: viral cultures and analysis (antigen detection and PCR) of other potentially affected body fluids (tracheal aspiration, urine, and stool) or mucosal sites (throat, nasopharynx, and rectum)
Consider: Brain biopsy in subjects with a progressive deterioration over time despite empiric therapy
4) Consider additional testing for selected patients based on exposure and travel history and other specific clinical symptoms.
Examples include but are not limited to the following
Culture or PCR of skin lesions if present for HSV, varicella zoster virus, and rickettsial infection
Naegleria fowleri (CSF wet mount and PCR) if swimming in warm freshwater
Bartonella (serum) and ophthalmologic examination if exposure to cats
Rabies serology (serum)
Treponemal testing (serum: rapid plasma regain [RPR] and specific treponemaltest)
Measles virus testing if unvaccinated
Tick-borne disease testing based on geographic region (ie, Borrelia, Ehrlichia, Rickettsia sp., and Anaplasma phagocytophilum serology)
Consider region-specific pathogens (eg, malaria based on travel history)
|
Table3. Common side effects for emergent- and urgent-therapy-phase anti-seizure medications. (adapted from the Neurocritical Care Society and American Epilepsy Society guideline for status epilepticus management)
| Medication |
Serious Adverse Effects |
Other considerations |
| Emergent/Initial Therapy Phase Medications |
| Lorazepam |
Hypotension, respiratory depression |
Dilute 1:1 with saline. |
| Diazepam |
Hypotension, respiratory depression |
Short duration, active metabolite |
| Midazolam |
Hypotension, respiratory depression |
Active metabolites, renal elimination, short duration |
| Urgent/Second Therapy Phase Medications |
| Phenytoin OR Fosphenytoin |
Hypotension, arrhythmia, purple glove syndrome |
Phenytoin is only compatible in saline.Fosphenytoin is compatible in saline, dextrose, and lactate ringers solutions |
| Levetiracetam |
Aggression |
Minimal drug interactions, not hepatically metabolized |
| Phenobarbital |
Hypotension, respiratory depression |
|
| Valproic acid |
Hyperammonemia, pancreatitis, thrombocytopenia, hepatotoxicity |
Avoid if possible hepatic dysfunction, metabolic disease, <2 years old with unknown etiology, pancreatitis, or thrombocytopenia |
| Propofol |
Propofol infusion syndrome (PRIS) |
Attention to PRIS, especially in young children; combine with benzodizaepine |
Table 4. Other Treatments for Refractory Status Epilepticus (RSE)
|
Advantages |
Disadvantages/comments |
| Other Pharmacological and Nutritional Treatments |
| Isoflurane |
Fast acting |
Possible neurotoxicity
Needs closed system, ie, gas recovery |
| Ketamine |
NMDA receptor antagonist |
Possible neurotoxicity; combine with benzodiazepines |
| Lidocaine |
Can rescue phenytoin-resistant RSE |
Cardiac monitoring needed; possible seizure induction |
| Verapamil |
Safe |
Does not have antiepileptic drug action; might improve availability of antiepileptic drugs in CNS |
| Magnesium |
Can enhance NMDA receptor blockade |
Possible induction of neuromuscular blockade |
| Ketogenic diet |
Safe |
Need skilled dietician; check for ketonuria |
| Immunological treatments |
Can act causally |
Formal exclusion of infection needed before treatment |
| Non-pharmacological options for RSE |
| Resective surgery |
Can act causally |
Not appropriate in multifocal status epilepticus; surgical risks |
| Vagal nerve stimulation |
Appropriate for long-term use |
Invasive procedure; cardiac arrhythmias rarely reported |
| Repetitive transcranial magnetic stimulation |
Non-invasive |
Possible seizure induction; need for sustained treatment |
| Electroconvulsive treatment |
Non-invasive |
Need for skilled interdisciplinary team; possible seizure induction |
| Mild hypothermia |
Acts on several pathophysiological mechanisms |
Usually only transitory control; avoid barbiturates (ileus) |
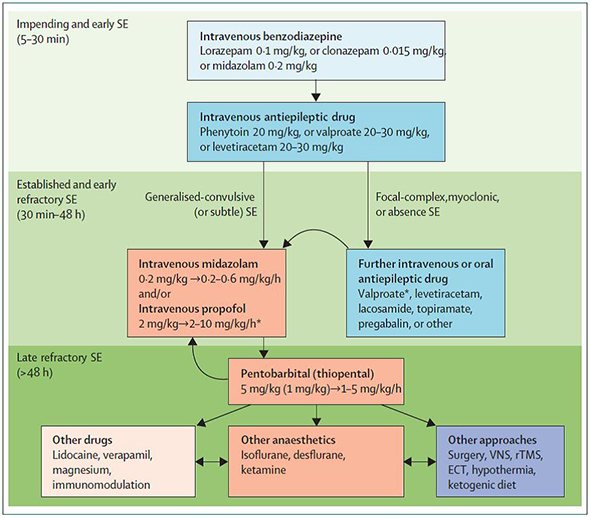 Figure 1. Flow of Status Epilepticus Treatment. Increasing refractoriness is indicated by the background green intensity. Light blue=first-line drugs. Dark blue=second-line drugs. Orange=third-line drugs. *Great caution is needed for use of valproate in children younger than 2 years (because of hepatic toxicity), and propofol in young children (because of propofol infusion syndrome). In this setting, benzodiazepines, phenytoin, and barbiturates are the most widely used options. (VNS=vagus nerve stimulation. rTMS=repetitive transcranial magnetic stimulation. ECT=electroconvulsive therapy. SE=status epilepticus) Figure 1. Flow of Status Epilepticus Treatment. Increasing refractoriness is indicated by the background green intensity. Light blue=first-line drugs. Dark blue=second-line drugs. Orange=third-line drugs. *Great caution is needed for use of valproate in children younger than 2 years (because of hepatic toxicity), and propofol in young children (because of propofol infusion syndrome). In this setting, benzodiazepines, phenytoin, and barbiturates are the most widely used options. (VNS=vagus nerve stimulation. rTMS=repetitive transcranial magnetic stimulation. ECT=electroconvulsive therapy. SE=status epilepticus)
|
| | |











